September 22, 2015 - Multiphase computed tomography angiography (CTA) proved reliable in determining the clinical outcomes of patients with acute ischemic stroke (AIS), according to a recent study published in Radiology.1
As part of the pilot phase of PRoveIT, a prospective observational study analyzing utility of multimodal imaging in the triage of patients with AIS, 147 patients underwent baseline unenhanced CT, single-phase CT angiography of the head and neck, multiphase CTA, and perfusion CT. Using multiphase CTA, researchers scored pial arterial filling on a six-point ordinal scale and tested interrater reliability. Clinical outcomes included a 50% or greater decrease in National Institutes of Health Stroke Scale (NIHSS) over 24 hours and 90-day modified Rankin Scale (mRS) score of 0–2. To predict outcomes, the researchers compared single-phase CT angiography, multiphase CT angiography, and perfusion CT using receiver operating curve analysis, Akaike information criterion (AIC), and Bayesian information criterion (BIC).
The results showed the interrater reliability for multiphase CT angiography was excellent. Although the ability to predict clinical outcome with curve analysis was modest, it was better than that of models using single-phase CT angiography and perfusion CT (P < .05 overall). With AIC and BIC, models that use multiphase CT angiography are better than models that use single-phase CT angiography and perfusion CT for a decrease of 50% or more in NIHSS over 24 hours.
The researchers concluded that multiphase CT angiography is a reliable tool for imaging selection in patients with AIS.
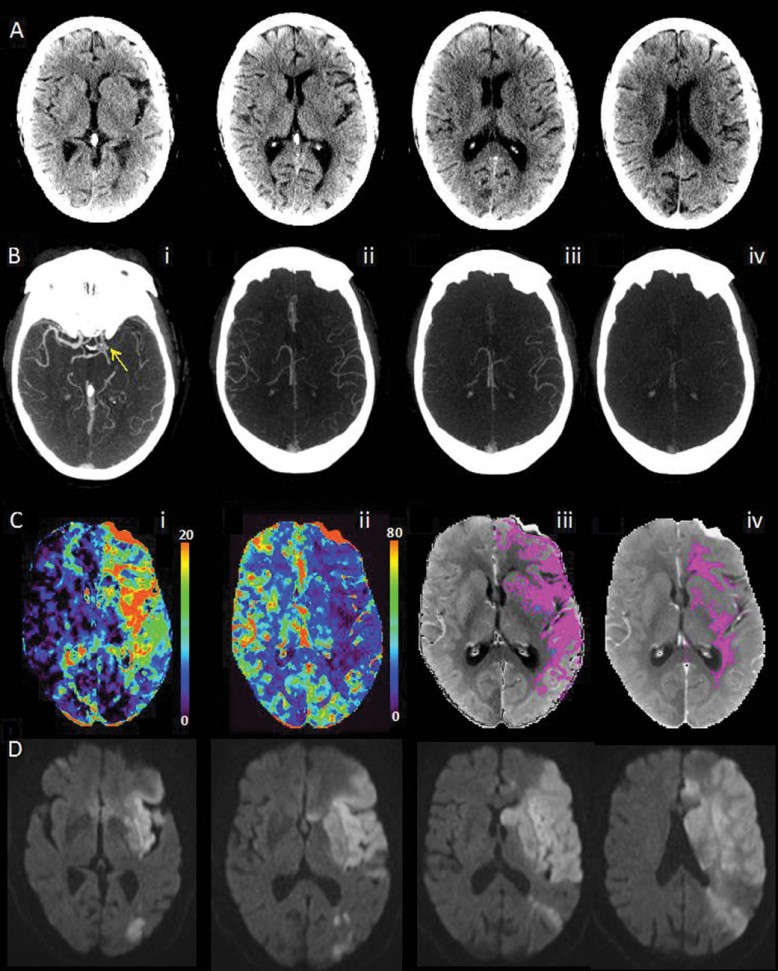
Image: Multimodal CT images obtained 2 hours 18 minutes after symptom onset in an 87-year-old woman with an NIH Stroke Scale of 15 and left hemisphere symptoms. A, Unenhanced CT ASPECTS score was 6. B, A proximal left M1 MCA occlusion (i). Multiphase CT angiography (three phases) maximum intensity projection images (ii, iii, iv) are indicative of one phase delay at worst, with similar extent and prominence when compared with the contralateral side. These indicate of a score of 4 and suggest the patient should undergo treatment. C, CT perfusion Tmax and CBF maps (i, ii). A CBF-defined infarct core is 1 mL (iii, no blue regions). A mismatch ratio of 106 and a small infarct core suggests the patient should undergo treatment. Multiphase CT angiography and perfusion CT imaging are congruent for treatment decision. D, MR diffusion images at 26 hours after admission show the final infarct as hyperintense. This patient did not attain recanalization with endovascular therapy. (Radiology 2015:257;2;510-520) ©RSNA 2015. All Rights Reserved. Printed with permission.2
Source:
- Menon BK, D’Esterre CD, Qazi EM, Almekhlafi M, et al. Multiphase CT Angiography: A New Tool for the Imaging Triage of Patients with Acute Ischemic Stroke. Radiology. DOI: http://dx.doi.org/10.1148/radiol.15142256
- Multiphase CT Shows Promise for Stroke Patients. RSNA.org. http://rsna.org/News.aspx?id=17320. September 1, 2015




